Insulin and diabetes: the present position
BY
Professor Charles H. Best, m.a., m.d., d.sc. (lond.), f.r.c.p. (Canada),
f.r.s. (canada), f.r.s.,
Professor of Physiology, University of Toronto.
(Verbatim report of the lecture delivered at the Annual General Meeting of the Research Defence Society, on Thursday, June 9th, 1938.)
I was very pleased to accept the invitation extended by your Committee to deliver the twelfth Stephen Paget Memorial Lecture. As a research worker I have, of course, always been in complete sympathy with the aims of the Research Defence Society. Your lecturer of last year, Professor Grey Turner, paid a very eloquent tribute, which I most heartily endorse, to the Paget tradition and to Stephen Paget in particular. I trust that the story of insulin, certain aspects of which I will attempt to relate to-day, may serve as a useful example of the advance of medical knowledge which may be secured by the appropriate use of the experimental method.
The early work on insulin in Toronto was based od the findings of many previous students of the subject. In this work most of these investigators had used dogs as experimental animals. In this species it is possible to remove completely or in part the pancreatic gland. This is done by surgical methods which are essentially similar to those now used by surgeons in operating on human beings when the pancreas is thought to contain some harmful tumour. The depancreatised dog was therefore the test object which made possible the discovery of the anti-diabetic substance. It is of considerable interest that only within the last few years have methods been made available by which we can remove sufficient pancreas from the rat or rabbit so that diabetes is produced in those species. This, of course, enhances the value of those animals for research in this field which has always as its ultimate objective the alleviation of human suffering.
The details of the investigations which led up to the isolation of insulin are familiar to a great many of you. The leading role played by Banting in the initiation and carrying out of the research must surely be apparent and cannot be over-emphasised. I would like to pay tribute at this time to the memory of Professor J. J. R. MacLeod, in whose laboratory the experiments were carried out and who made possible the rapid extension of the findings which Banting and I were able to obtain in the spring, summer, and early
autumn of lit'il. I was invited to collaborate in this research for two reasons, 1 suppose : first, because during the previous year I had been working with Noble, studying the pathway of those nervous impulses which may produce a transient diabetes, thus making me familiar with the chemical methods used in investigating carbohydrate metabolism, and, secondly, because I had already made arrangements with Professor Macleod to spend a further year in his department to secure a Master's Degree in physiology.
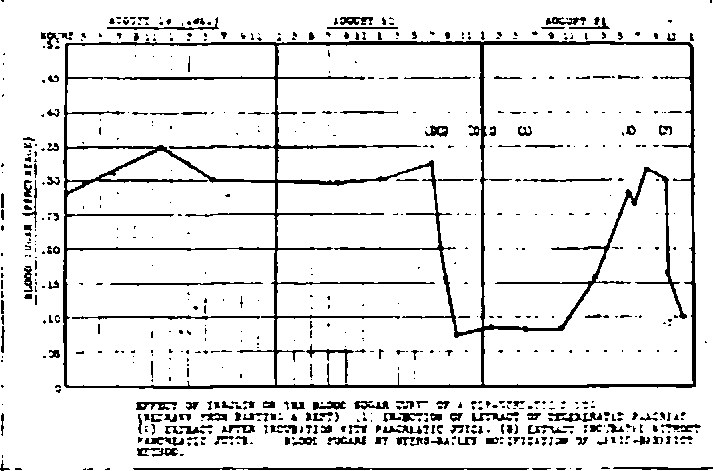
I can illustrate some of the early findings in these researches by a few-lantern slides. The first is a chart (Fig. 1) illustrating the blood sugar value
Fic. 1.
normally and after the removal of the pancreas. Here I should like to point out the great contribution which the biochemists made in elaborating a reliable method for the determination of the sugar in very small samples of blood. This was certainly one of the most important factors in the success of an investigation of this kind.
I next show you a picture (Fig. 2) of the first dog whose life was prolonged
by the administration of the anti-diabetic substance. This animal lived for some ten weeks and remained in excellent condition. It made a real contribution, I believe, to the advancement of this subject.
In 1922, Banting and I decided to prepare enough insulin for clinical trial. One of our first attempts was made by administering gallons of solution of a substance known as secretin to in anaesthetised ox. We thought by this procedure we might exhaust the enzymes of the pancreas and then by performing a pancreatectomy have available larger supplies of insulin. We removed the organ and did make some active extracts from it. As I look back on that futile but gallant attempt I think an alternative tide for the thesis might be : " Lost among the stomachs of the ox." We visualised at that time rows and rows of oxen each receiving secretin to eliminate enzymes from the pancreas, and large amounts of anti-diabetic materia! being made available from their organs. It became obvious, however, that this was not a practicable proposition. We then resorted to the use of alcohol as an agent for the precipitation of inert material including the enzymes, ir.d our efforts immediately met with considerable success. One day we made a special lot of this material from the pancreas of one beast. The pancreas was removed aseptically, and the extract tried first on our colony of depancreatised dogs and then on ourselves. As the effect on Banting and me was only local, we decided to go ahead with the administration to a severe case of diabetes, and this was done on January 11th, 1922. The patient was one Leonard Thompson in the wards of Toronto General Hospital, under the care of Dr. Walter Campbell. He received his first injection on that date and subsequently was kept as far as possible under the influence of insulin. He was not a particularly co-operative patient and often threatened to spoil his very interesting history by motor-cycle accidents and things of that sort. Fig. 3 shows Leonard Thompson ten years' after the commencement of insulin treatment.
Soon after this, improvements in the method of preparation of insulin were made by Professor J. B. Collip, who was the first to join us in the new series of researches. Very soon a number of patients suffering from severe diabetes were under treatment. But then the art—for it certainly was not a science—of making insulin was lost, and some of these patients, who had been rescued from coma lapsed again into that state, some of them dying through lack of insulin. It was a matter of very great difficulty to find again the procedure which gave us potent extracts, and I am afraid, as we look back on it, that in attempting to recover the position it would have been much better had we spent some time thinking over the matter properly, perhaps going for a gallop in the country, preferably on horseback, instead of setting to work immediately on experiments.
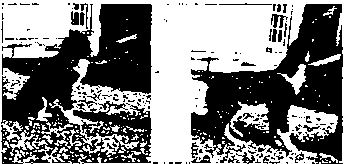
My next slide is the only other one of a human being that I have to show you. It is the picture of a little boy who played about in the laboratory at a time before insulin was really available. His diabetic condition was such as you see on the left-hand side of the picture, and a year later he had . recovered, so that he looked the healthy little creature that you see on the
other side. I show him because, after all, at that lime we were not seeing patients, but we did see a lot of this little boy, and his recovery was a matter of very great pleasure both to Banting and to me. In spite of this dramatic improvement which takes place there are some people who would go so far as to withhold insulin from a diabetic child—always the child of someone else. They are stoics over the pain of others, and never yet have I come across anyone who had the courage of his convictions to a sufficient extent to withhold insulin from his own child.
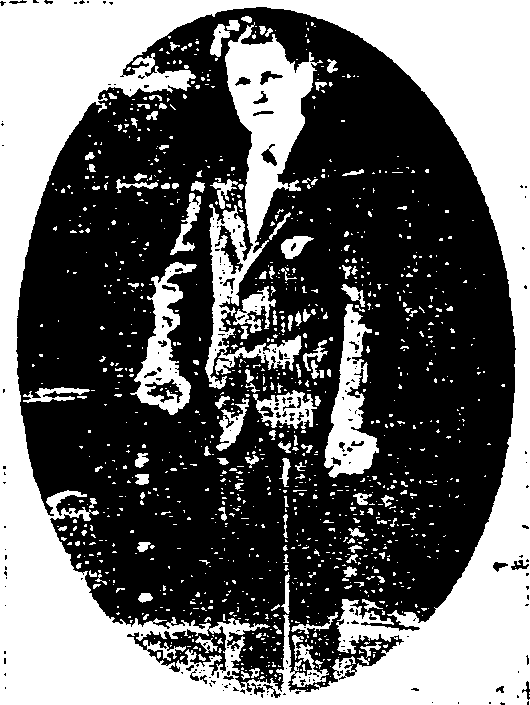
Fig. 3.—Leonard Thompson, fir,: pnticnt to receive insulin (Jan. 1 1th. 10-2). Photograph taken ten years later.
Happily, now the preparation of insulin is on a much more secure scientific basis. Facilities for the large-scale production of this material were first made available in the Connaught Laboratories which were under the direction of Dr. J. G. Fitzgerald, and through this co-operation, and later that of the pharmaceutical companies, the amount of insulin gradually increased until finally an adequate amount was always obtainable.
I must not take time in describing the primitive apparatus which we used in the early stages of large-scale production. Some of you have seen the gigantic wind tunnel. We used the fan from one of the large university buildings and this was attached to the tunnel in which we put trays of acetone extracts of the pancreas. I can still hear the roar of that thing as we concentrated the extracts. The next stage was the use of a still with a circular tube condenser, and 1 remember very well the sturdy little Englishman whose duty it was to put two or three tons of ice each day in that condenser. He eventually left; he must have felt it very futile to put the ice in it only to melt into water and flow away again.
I want now to give you a very brief description of the present methods which are used in the preparation of insulin on a large scale. Unfortunately, the idea of preparing a colour film for this purpose only occurred to me a few days before I left Toronto, and the film was pressed into my hands an hour before the boat train left. However, if I explain a little beforehand, you may find a more intelligent interest in the film I am about to show. It begins with some shots of the Medical Building of the University, put in, I suppose, to provide a little atmosphere. The second story of this building was the Department of Physiology, and you will see on the film a black smudge which is supposed to represent the bench assigned to Banting and me. A very good bench it was but it does not photograph very well.
Then we go to the Connaught Laboratories and see the masses of beef or ox pancreas brought in and minced through a large chopper. Alcohol and acid are added, and the whole is stirred up to extract the insulin, which is soluble in the liquid. The gland residue is separated iVom the liquid in a centrifuge, which you will see whirling about, and then the liquid goes through a filter press which clarifies it. Eventually we see the clear solution containing most of the insulin from the gland coming from the funnel of the filter press. This goes to large vacuum stills where it is concentrated to a small volume, and afterwards the filtrate is drained out of these stills. Salt (sodium chloride) is added, and all the insulin obtainable by that procedure from 2,400 lb. of pancreas floats to the top of the solution in a bulk of a pound or two. This material is then taken to a small chemical laboratory where it is fractionated and purified by various procedures. It is passed through a filter, the pores of which are small enough to remove bacteria but large enough to allow the insulin molecule to pass through. It is then tested on mice for potency, and filled into sterile phials, packaged, and made ready for delivery.
The unfortunate thing about the preparation of insulin nowadays is that the cost of the containers is such a large fraction of the total. Thus, even though the yield is increased there is very little lowering of the price. Then! towards the end of the film, we see a depancreatised dog which had received insulin over a long period and is very active or. ::, and at last we see the Medical Building again—I suppose because the photographer took too much of it to begin with and snipped it off and put a little of it at the end !
(Professor Best then showed the colour film, the sequence of which he • had just described.)
He continued : If I may speak for one moment *•« more scientific members of the audience, the dog shown in this film is interesting from other points of view. In confirmation of the work carried out by Dr. F. G. Young at the National Institute for Medical Research, Dr. James Campbell and I produced permanent diabetes in dogs by the administration of pituitary extract. This dog was made permanently diabetic as a result of such injection, and afterwards its pancreas was completely removed. It was only slightly more diabetic after the operation than it had been before, and we can confirm the findings of Richardson and Young that degeneration of the islet tissue was found and, furthermore, the insulin content of the pancreas was negligible. You can see from the film that the dog is in excellent condition. It was diabetic as a result of injection of pituitary extract, and now that it has no pancreas it remains quite happy with its daily injections of insulin.
I have next to show you the insulin content of pancreas obtained from the animal at different ages. The data given in Table I are from the work of Scott and Fisher.
Table I.
Insulin Content of Pancreas in Cattle of Various Ages.
Results of Biological Assays
Description of Cattle. (international units per gm. pancreas).
|
|
Sample 1. |
Sample 2. |
| Sample 3. |
Average. |
|
Foetal calves, under o months |
29-2 |
38-8 |
i 31-7 ' |
33-2 |
|
5-7 |
23-2 |
24-9 |
! 21-1 |
23-1 |
|
Calves, 6-8 weeks (milk diet) |
12-8 |
10-4 |
j 10-9 ! |
11-4 |
|
Cattle, 2 years |
3-9 |
|
4-5 |
4-S |
|
Cows, 9 years and older ... |
1-7 |
2-0 |
1-8 |
1-8 |
|
" .. .. (pregnant) |
2-0 |
2-2 |
• 2-3 |
o.o |
The insulin content is much greater during intra-uterine life than after birth, and we took advantage of that fact in the early work on insulin, although we did not know it, for foetal pancreas was the source of insulin for quite a long period. As the animals get older the insulin content of the pancreas diminishes, and the organ is not such a potent source of active material.
Efforts were made in many laboratories to purify the insulin. The goal of the chemist was finally reached in 1926 when the late Professor Abel, of Johns Hopkins University, obtained insulin in crystalline form (Fig. 4). The crystals do not always take the same form. The potency is always the same and has been set at 22 units per milligramme. Harington and Scott worked on the subject in London, and Scott after his return to Toronto made large amounts of crystals and eventually was able to show that zinc was necessary for the formation of the crystalline substance.
The test tubes which I show you contain insulin in an amorphous state, not crystalline, and I also show the appearance of the same preparations after a small amount of zinc had been added. By this research Scott changed the preparation of crystals from an art to a science, and insulin can now be prepared in crystalline form in any amount desired. Curiously enough, previous to this work, the people who had the purest insulin found the greatest difficulty in preparing crystals while those who had relatively crude insulin did not have this trouble, presumably because zinc or some closely related metal was present in the preparations.
The international yardstick of insulin is this crystalline preparation, ft is stored for the Health Organisation of the League of Nations, in part in what we like to think of as the Central Laboratory of the British Empire, the National Institute for Medical Research at Hampstead. and in part in Toronto. I could dilate on the work of the Standards Commission of the Health Organisation, but this is not an appropriate place to do so. It has
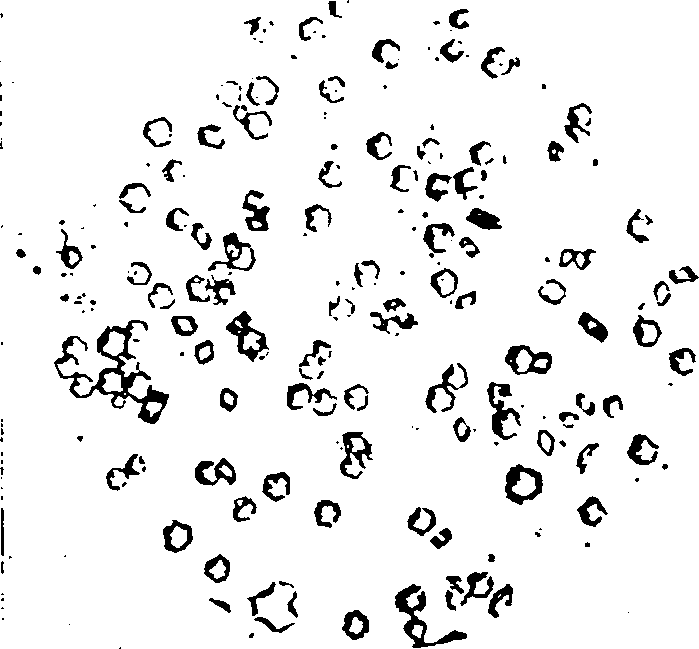
Crystals of Insulin
Fic. 4.
certainly brought order out of chaos in this field and in many others by-setting up these standards.
I am sure my colleagues would be somewhat shocked if I were to state that the action of insulin is to remove all the signs and symptoms of diabetes. That is a complete but superficial definition. To be more specific, insulin accelerates the formation of a complex sugar which is apparently necessary for the proper functioning of the animal organism. It increases slightly the combustion of sugar in the body and it prevents the wasteful formation of excess amounts of sugar from other substances.
A great many efforts have been made to prolong the action of the substance. I will spend no time on the preliminary attempts, but I may remind you of the great success achieved by Professor Hagedorn and his colleague in Copenhagen by the use of protamine uhich, when combined with insulin, forms an insoluble substance absorbed slowly from the tissue spaces. This has been shown in many cases of diabetes, but it can be shown excellently in rabbits, where the delayed-action is seen in contrast to the more rapid and evanescent action of the ordinary material. It can be seen perhaps even better in the dog, where the ordinary insulin has an effect of a certain duration while the same dose of the protamine-insulin has an effect much more prolonged (as shown in Fig. o). This means, of course, in many
cases of human diabetes fewer injections per day. Something of the same effect can be secured with zinc alone. This work of Scott and Fisher was in progress in Toronto when the Danish investigations were reported. From the charts I am able to show you will observe the contrast between insulin with zinc, where the effect is delayed, and the more rapid and transient effect of the insulin by itself. Here again the effect of zinc is shown in the longer time before the blood sugar begins to come down, but when it does come down it stays down for a long time in contrast to the brief action of the ordinary material. It was subsequently shown by Scott and Fisher that a mixture of protami-- -rid zinc with the insulin possesses certain advantages over the protamine-insulin used alone. One advantage is that the suspension of the protamine-insulin mixture in solution is much more stable when a trace of zinc is present. It will be seen from a comparison of these two phials containing protamine and insulin that in the one without zinc a large pan of the substance separates out and sticks to the glass, whereas the one with a trace of zinc remains perfectly and permanently homogeneous and stable.
Another effect is that -».inc prolongs still further the absorption of the active material. Therefore in North America protamine-zinc-insulin has largely supplanted protamine-insulin. At the present time approximately
one. I am not sure whether this is worth while or not. More recently a group of workers in the United States have prepared a protamine-zinc-insulin which is clear and which still has a delayed action. This will possess certain obvious advantages in that it can be sterilised as a solution and eliminates the danger of uneven sampling from the bottles. Perhaps it has other advantages as well. We believe, from the data we have seen so far, that the duration of the effect is not quite as great as that of the suspension, but still it may be sufficiently prolonged to make it a useful preparation.
I next show two curves which indicate the difference between one injection of protamine-zinc-insulin where a low blood sugar is maintained in a depancreatised dog throughout the day in contrast to the effect of one injection of the ordinary material. Of course, a clinician treating a patient would not give only one injection, but this does serve to emphasise the contrast.
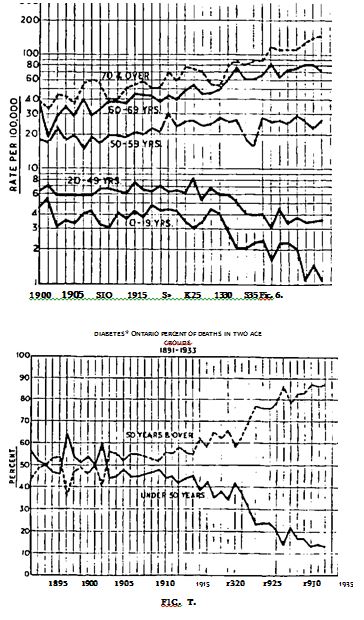
I come now to another aspect of the subject, namely, diabetic mortality. In Ontario this is particularly interesting, because there is no other place in the world where everyone who wished to have it has had insulin available from 19*22 onwards. It is perfectly true that in certain age groups the mortality from diabetes is not coming down, it may even be going up, because there are now many more diabetics who reach the older age groups. When these people die, as even the diabetic must, the cause of death is usually stated to be diabetes. But in the earlier age groups, from birth to 19 years, the sharp decline is obvious, and again the difference in the mortality as between those under 50 and ov^r 50 is very significant. The evidence as to the effect of insulin is perfectly convincing, and is clearly shown in Figs. 6 and 7, for which I am indebted to Dr. R. D. Defries.
In the next slide I give figures showing the distribution of insulin in Canada, starting from 1922 and continuing, of course, at a very low level in 1923 and 1924. The curve is still going up sharply (Fig. 8). This means that more and more insulin is being used each year. Some of you who are associated with business have already looked, I daresay, for a dip in the curve in 1929-31, the period of economic depression in North America, but there is no such dip, proving that insulin is not a luxury. The interesting thing, too, is that the curve becomes steeper and steeper, which obviously means that while the older practitioners did not use much insulin, the younger ones, trained in more modern methods, tend to use this preparation as well as many other therapeutic substances to a greater extent.
In conclusion, I think that the attention given me by this large audience this afternoon means that they are interested in carbohydrate metabolism, and yet we have a great many different groups represented here. I am very much flattered by the attendance of a number of research workers in this field, and I know they will agree with me when I say that there is much more for all of us to do in relation to this problem. To the medical students present I would say that they .need not bother to read all the 10,000 publica-• tions that have appeared on insulin since 1922, but they will perform their most valuable function by spreading the modern knowledge of the treatment
jo
of diabetes and other diseases throughout the country. Lastly. I trust that the diabetics—I know that a number are here to-day—will feci that definite advances in the treatment of their condition arc steadily being made. I
TOTAL UNITS OF INSULIN DISTRIBUTED ANNUALLY BY CON NAUGHT LABORATORIES.
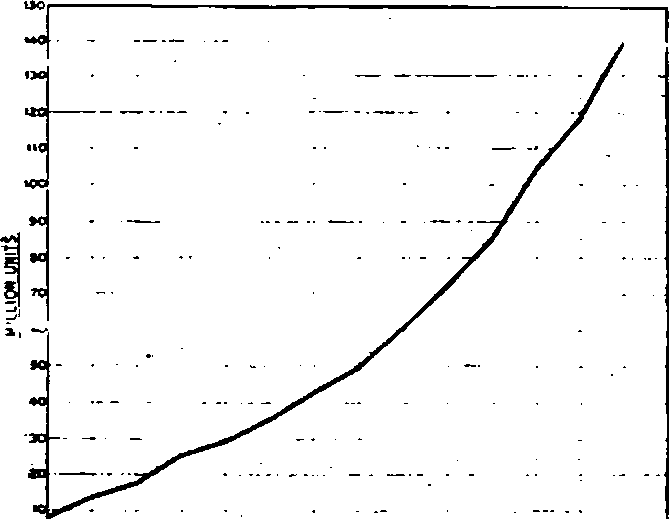
Fig. 8.—Distribution of Insulin in Canada from 1923-1937.
thank you, Air. President, for the honour you have conferred on me in asking me to give this lecture.
(The Chairman then called upon Sir Edward Mellanby to propose the vote of thanks to Professor Best.)
Sir Edward Mellanby : I regard it as a great privilege to have been invited to propose this vote of thanks to Professor Best. To me in any case, and I expect to everybody in this room, this occasion has been a great intellectual treat. To sit in a fine lecture room with a very large audience and to hear a lecture which technically has been excellently delivered, on a subject which affects the lives of thousands of people, by one who himself has played a large part in the initial work on the subject is a very happy experience. It almost makes one feel that the world is a good place. Yet there is one fly in the ointment, to think that it is necessary for scientific men to come and justify the use of animal experiments. That indicates to me that after all, this world is not so perfect.
It has been my lot to attend patients suffering from diabetes before the discovery of insulin and also to look after many since that discovery. It is almost impossible to convey a real appreciation of the difference in outlook of a medical man in regard to these cases as between those two periods or to describe the mortification with which in the pre-insulin era one approached
the ordinary diabetic lying in his bed when one knew that whatever one did one could only lengthen his life by a few weeks or months. To-day, one approaches the diabetic almost with a jaunty air, knowing that one can turn him out to do a normal job of work within a few weeks. It was also my lot to be one of the first people in this country not only to use insulin but to make it in the laboratory. Those were days of some excitement, and I can apprtciat'. :hk ir.icnsc filings which Banting and Best must have experienced when they did their first clinical tests.
I remember my first two patients who were treated 15 or 16 years ago. Both are alive to-day and perfectly well. One of them was a man over six feet in height who was brought in apparently moribund. He weighed only six stone, and could not walk or stand. That man left hospital after a month or two, and he became chairman and managing director of one of the most successful steel companies in this country—a company, I may add, which even paid a dividend during the worst part of the depression. He is living a healthy and complete life. The other patient was a boy of 16 who is now-living an entirely healthy life as a market gardener.
That was my own experience, and since then medical men are seeing thousands of diabetic patients, most of whom can live excellent lives if they will only do what they are told. Yet this is only one of many advances made in recent years. In the case of some diseases we have discovered by animal experiment not only the cure and control of the disease but have made such advances in knowledge that we can actually prevent the diseases from occurring. This is the kind of medical knowledge which tends to be forgotten. It is a curious situation that the more successful we are in medical research the more likely are the public to forget all about it. These diseases which have killed hundreds or thousands of people disappear, and the work which has resulted in their prevention goes out of the public mind. The work we have heard described this afternoon, however, has not only tremendous practical importance, but great dramatic interest. It has been the means of bringing people who were on the very edge of the grave back to a normal life. Professor Best has described the work excellently, and everyone here will wish to congratulate him on the part he has played in this wonderful discovery.
Dr. R. D. Lawrence : I am very glad to have the opportunity of seconding this vote of thanks. Sir Edward Mellanby has expressed our feelings from a more scientific point of view, but I have no doubt that the reason why I am asked to speak is because I represent the average pretty healthy diabetic living on insulin and saved by Banting and Best. How do we know that there are diabetics in this meeting ? I can only say that if you look round the company and see an individual who looks rather healthier than anybody else it is very likely that he is a diabetic living on insulin. We are tremendously indebted to Banting and Best.
The Chairman at this point invited questions and one lady questioned Professor Best on the possibility of preventing early diabetes appearing and whether the mild diabetic should take insulin. Professor Best said at last, in reply to her insistent inquiries, that if he were in her place he would go to a good medical man. As she still persisted in her questions he said that he would see a second medical man, and finally, when she urged him to give his own opinion on the case in point, he replied, amid laughter, that he was not licensed to practice in England.
In reply to another speaker, Professor Best mentioned that in Canada and the United States, on the basis of the insulin distributed, and assuming a daily dose per individual of 35-40 units, some '2-2O,0OO people were taking insulin regularly.
The vote of thanks was then put to the meeting by the Chairman and enthusiastically accorded.
On the motion of Professor A. V. Hill, a further vote of thanks was accorded to Lord Lamington for taking the chair. It was mentioned that Lord Lamington had come several hundreds of miles to attend the meeting, and Professor Hill expressed the affectionate regards of the Society for their President, and the gratitude for the interest he took in its affairs.
THE BUSINESS MEETING.
The Business Meeting followed immediately after the Stephen Paget Memorial Lecture, Lord Lamington again presiding.
The Vice-Chairman (Professor A. V. Hill) presented the Annual Report of the Committee, which had been circulated, and formally proposed its adoption. This was seconded by Sir Henry Dale and, on being put to the meeting, was carried unanimously.
The Ch-urnlajs" then called on Sir Leonard Rogers to present the Hon. Treasurer's Report for 1937.
Sir Leonard Rogers said that his tenth report as Honorary Treasurer was a little more cheerful than usual. The ordinary income from donations and subscriptions had increased by £41, and two generous bequests, in the one case of £300, and in the other of £100, had been made respectively by the late Mr. Arthur Wilson and Dr. Emerson Lee. As a result there was a balance on the year's workings, but approximately £64 went towards the deficit on the previous year and £63 towards the deficit of the year before. After deducting these sums and allowing for contingencies in 1938 the Society was still left, however, with £150 for investment, and the total assets now stood at £3,035, which was the highest in the history of the Society. He had made a special appeal in his report for small legacies. If only one-hundredth of the amount of the legacies received by anti-vivisection societies came to the Research Defence Society it would be able to carry on the work of defending research, seeing that the strength of its case was one hundred times better than theirs. He wished this could be brought home to the kind-hearted ladies, mostly belonging to a generation before girls were taught science, who did so much to finance the opposition and thereby
Last edited: 19 January 2018 13:56